
Still relatively unknown and widely underdiagnosed, andropause is nonetheless a very real phenomenon. Also referred to as “age-related androgen deficiency” (ARAD), it describes the gradual decline in testosterone levels in aging men. While not systematic, andropause comes with various symptoms that require attention to prevent complications. Dr. Michel Mouly, a gynecologist, surgeon, and oncologist based in Paris, sheds light on the topic.
While menopause has become an increasingly discussed subject, andropause remains largely taboo. The reason? It affects testosterone, the very hormone associated with masculinity. Acknowledging its decline means accepting that one’s strength and vitality are not what they once were, in a society where virility still holds great importance. In reality, andropause affects between 10% and 20% of men over 50, and between 50% and 70% over 70. In other words, testosterone deficiency becomes more common with age, though its impact varies from man to man.
Several factors influence the onset of ARAD, with lifestyle being a key component. “It’s important to keep in mind that male life expectancy is increasing. Today, it stands at 80 years, compared to 73 in 2000. This means that hormone deficiency will affect a growing number of men. If this trend continues, we might assume that by 90 or 100 years old, nearly all men will experience ARAD—just as 100% of women undergo menopause around their fifties,” explains Dr. Mouly.
It’s a significant issue that is still rarely discussed. Yet, just like women, men experiencing hormonal deficiencies need proper monitoring and care. In fact, Dr. Mouly is set to release a new book in May on the subject. Titled Hormones: Life Begins at 50!, the book is co-authored with Dr. Carol Burté, an andrologist specializing in sexual medicine.
Andropause: the male menopause?
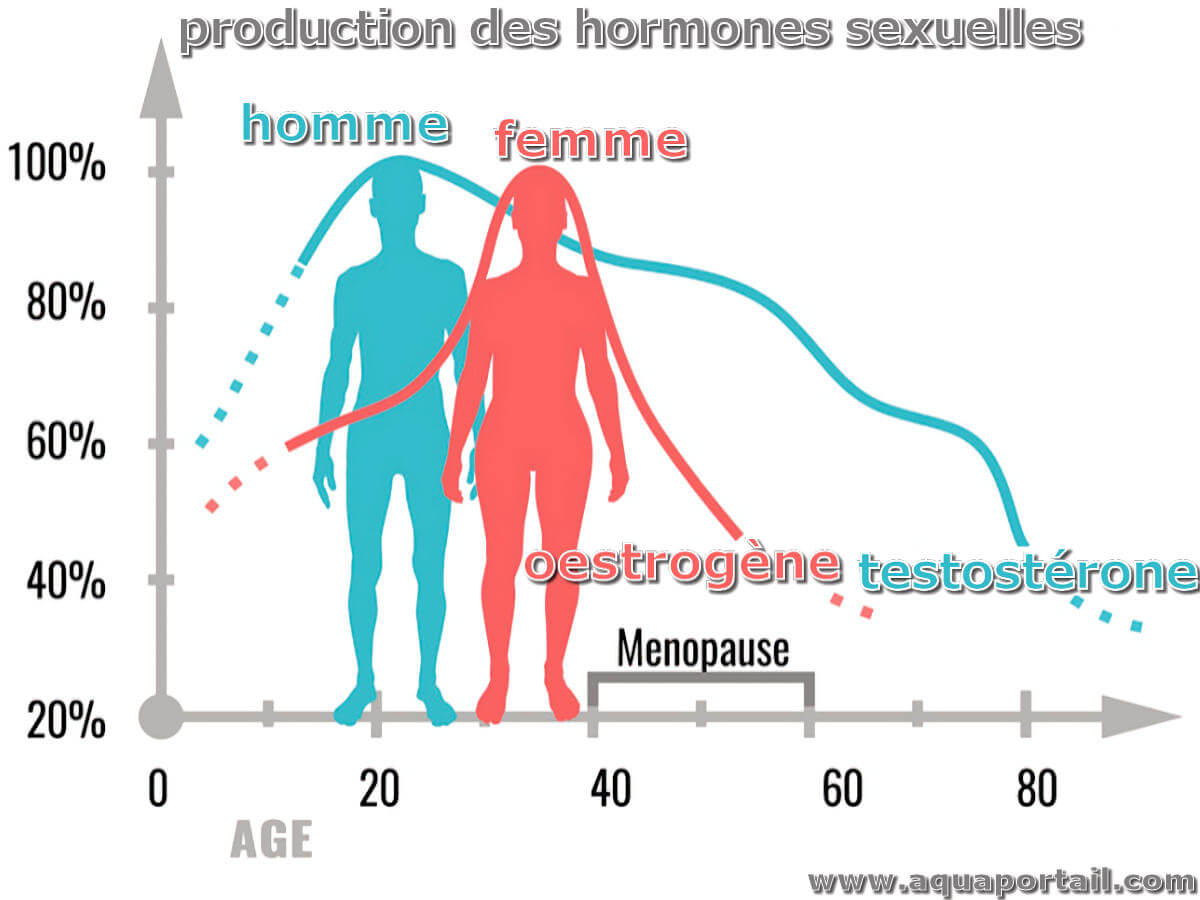
While menopause was first medically described in 1816, research on the effects of male hormonal aging only began in the 1940s. The term “andropause” gained popularity in the 1980s and 1990s. Often seen as analogous, , these two phenomena actually differ in several ways. “Menopause, or age-related estrogen deficiency (ARED), marks a sudden and complete halt in estrogen production in women, occurring over just a few years. In contrast, testosterone deficiency (TD) or age-related androgen deficiency (ARAD) is a slow and gradual process that can span decades. It is not a complete shutdown of hormone production as seen in women,” explains Dr. Mouly. “Testosterone levels begin to decline as early as age 30, at an average rate of 1% per year. This decline becomes more pronounced after 50 and even more so after 70, where symptoms can become more noticeable and debilitating,” he adds.
 However, not all men experience hormonal decline in the same way, as multiple factors come into play. A sedentary lifestyle, poor diet (smoking, alcohol, junk food, excessive sugar, and vitamin deficiencies), obesity, oxidative stress, lack of sleep, and chronic illnesses all accelerate the process. Long-term medication use, such as corticosteroids or certain antidepressants, can also lower testosterone production. “Elite athletes, men with a healthy lifestyle, and those with favorable genetics can maintain optimal testosterone levels until their 70s or 80s. Conversely, an overweight, stressed, and inactive man may experience deficiency as early as his 50s,” the doctor explains.
However, not all men experience hormonal decline in the same way, as multiple factors come into play. A sedentary lifestyle, poor diet (smoking, alcohol, junk food, excessive sugar, and vitamin deficiencies), obesity, oxidative stress, lack of sleep, and chronic illnesses all accelerate the process. Long-term medication use, such as corticosteroids or certain antidepressants, can also lower testosterone production. “Elite athletes, men with a healthy lifestyle, and those with favorable genetics can maintain optimal testosterone levels until their 70s or 80s. Conversely, an overweight, stressed, and inactive man may experience deficiency as early as his 50s,” the doctor explains.
Signs and symptoms
So how can one tell if they are experiencing andropause? “Symptoms are not always easy to identify because they develop gradually. Yet, they can deeply impact quality of life and relationships. Key warning signs include the disappearance of morning erections and erectile difficulties (less firmness, slower onset); weaker ejaculation and reduced pleasure; persistent fatigue and slower recovery after exertion; abdominal weight gain and muscle loss; decreased libido and fewer erotic thoughts; mood swings, irritability, anxiety, or even depression; sleep disturbances, night sweats, and hot flashes,” lists Dr. Mouly.
Many prefer to ignore these signs, attributing them to fatigue or everyday stress. To cope, some men turn to exercise or erectile stimulants (yes, the famous blue pill!).
“Andropause is still widely dismissed—partly due to a lack of awareness among doctors who rarely bring up the subject in consultations, but also because of cultural taboos. Society values strong, virile men, and admitting a drop in testosterone is seen as acknowledging a vulnerability, often perceived as a blow to masculinity. There is also the notion of ‘medical cheating.’ For example, while women immediately feel the effects of hormonal deficiency, men compensate with the blue pill, which masks the problem rather than treating it,” says Dr. Mouly.
What are the treatment options?
Just like menopause, andropause can be managed with treatments designed to counteract the adverse effects of hormonal decline. “The goal is to restore optimal testosterone levels to regain energy, muscle strength, and sexual desire. There are two main options: a transdermal gel applied daily to the skin, usually on the shoulder, and long-acting intramuscular injections administered every two to twelve weeks,” explains the doctor.
Before starting any treatment, it is crucial to undergo rigorous hormonal testing twice, including assessments of free and bioavailable testosterone, SHBG (Sex Hormone Binding Globulin), prostate cancer screening (PSA), and hematocrit levels (to monitor polycythemia risk). Experts recommend an initial test around ages 40-45 to establish a baseline.
Some men naturally have high testosterone levels, meaning even a moderate drop can lead to clinical symptoms despite test results remaining within normal ranges. Conversely, a man with naturally low testosterone may experience no symptoms at all and may not require treatment.
What about side effects?
As you’ve probably gathered, a testosterone decline is no small matter. Beyond causing chronic fatigue, depression, and lack of motivation, it also increases cardiovascular risks (hypertension, atherosclerosis), reduces bone density (male osteoporosis), leads to muscle loss with fat gain, and impairs cognitive functions such as memory and concentration. This is why treatment is essential when necessary. “As long as levels are kept within the normal range, adjustments are made gradually, and regular monitoring is in place, there are no risks. On the contrary, most men start feeling better within just a few weeks of treatment,” reassures the doctor.
“In fact, the French Association of Urology (AFU) now recommends more systematic screening for testosterone deficiency,” adds Dr. Mouly. “Yet, treatment remains limited. Doctors can be hesitant to prescribe hormone therapy due to lingering controversies. But contrary to common belief, testosterone does not cause prostate cancer. The AFU even confirms that it can be prescribed after prostate cancer if the prognosis is favorable. There is a severe lack of public awareness and information campaigns. Ultimately, the pharmaceutical industry prefers selling Viagra over treating the root cause with testosterone.” According to the specialist, men should consult a doctor as soon as they notice a loss of morning erections, rather than immediately turning to erectile dysfunction medications.
“With life expectancy on the rise, it is crucial to help men reconnect with their physiology and provide them with appropriate care. Testosterone deficiency is not inevitable—there are solutions to maintain health, vitality, a fulfilling sex life, and, by extension, a happy relationship. At 50, life is just beginning!” concludes Dr. Mouly.
Picture (c) : kith
